Things are changing.
We are shifting from a forensic psychology non-solution to a clinical psychology solution for complex family conflict surrounding divorce.
This is not a child custody issue. The conflict surrounding child custody is a symptom. The issue is family pathology that is creating complex attachment-related pathology in the family; complex family conflict surrounding divorce.
This is a family pathology and treatment issue. Conducting family therapy is the domain of clinical psychology, treating attachment pathology in the family is the domain of clinical psychology (a child rejecting a parent is an attachment-related pathology), treating the expression of parental personality disorder pathology in parenting and the family is the domain of clinical psychology, and treating the trans-generational transmission of complex trauma is the domain of clinical psychology.
This is a clinical psychology issue, diagnosing and treating family pathology; the attachment system, family systems therapy, personality disorder pathology, complex trauma. Clinical psychology.
The DSM-5 diagnosis for pathogenic parenting that is creating significant psychopathology in the child is V995.51 Child Psychological Abuse. Diagnosing and treating child abuse is the domain of clinical psychology. This is not a child custody issue; it’s a child protection issue.
The clinical psychology concern is the significant degree of psychopathology being created in the child by the pathogenic parenting of the allied narcissistic-borderline personality parent… assessing, identifying (diagnosing), and treating psychopathology is the domain of clinical psychology.
Following divorce, a spouse is using the child as a weapon of revenge and retaliation against the other spouse-and-parent in the divorce, in order to inflict severe emotional abuse and the psychological trauma of losing their child on this targeted spouse-and-parent. This pathology is a form of domestic violence (Intimate Partner Violence; IPV), the emotional abuse of the ex-spouse using the child as a weapon of spousal revenge and retaliation for the divorce, and in the process psychologically abusing the child by creating severe pathology in the child.
The assessment, diagnosis, and treatment of Intimate Partner Violence (IPV; domestic violence) and child abuse is the domain of clinical psychology.
This is not a child custody issue. The child custody conflict is a superficial symptom of much deeper clinical pathology in the family. The issue is one of psychopathology, that’s the domain of clinical psychology. The clinical psychology argument package represents the return of clinical psychology to court-involved consultation, court-involved assessment of pathology, and court-involved treatment of pathology.
Identification of pathology is called diagnosis. Assessment leads to diagnosis, and diagnosis guides treatment. Treatment solves conflict and restores the child’s healthy family context and healthy development.
We are shifting the legal argument package that is being presented to the court. Parents and their attorneys will be asking the court for a clinical psychology assessment of family pathology, not a forensic psychology assessment for child custody.
The Forensic Package
Up until now there has been only a single option for parents and their attorneys, the forensic psychology legal argument package that frames the issue as one of custody and visitation. That has changed. There is now an alternative approach; a treatment focused approach from clinical psychology.
The clinical psychology legal argument package is grounded on a different set of constructs from professional psychology (Bowlby; Minuchin; Beck) than is the forensic psychology argument package (arbitrary and unknown foundations), and the clinical psychology option seeks a different remedy from the Court than the forensic psychology argument package.
Since the focus of the forensic psychology legal argument is on child custody, the initial forensic psychology remedy moves inexorably into a “child custody evaluation” as the only means to obtain the input of professional psychology into the question of the child’s non-compliance, and potentially influenced child behavior regarding compliance, with the custody visitation orders of the court.
The task of each parent then becomes proving their position regarding the child’s rejection of a parent to the child custody evaluator, who will decide on the “evidence” presented to the custody evaluator on the relative merits of each party’s position, and will decide on the custody and visitation schedule for the family – thereby ABROGATING the duties of the judge… to hear argument and evidence, to make a determination of fact, and to render a decision regarding the custody visitation schedule.
All done by the custody evaluator – not the judge. The judge may either then accept or reject and alter the ruling of the custody evaluator – typically without benefit from a second opinion from professional psychology regarding the family symptoms and family pathology.
Custody and visitation decision-making has essentially been assigned out of the courts and to forensic psychology, and the only approach available from forensic psychology is an invalid (no inter-rater reliability) six- to nine-month forensic child custody evaluation costing between $20,000 to $40,000.
Each parent tries to influence the custody evaluator to their position. The position of the allied parent (supported by the child) is that the targeted parent is “abusive” and “deserves to be rejected: by the child. The position of the targeted parent is that the child’s attitudes and behavior is being influenced and controlled by the allied parent as a means to inflict emotional suffering on the targeted parent for the divorce (that the child is being used as a weapon of spousal revenge and retaliation for the divorce).
The custody evaluator meets with everyone to hear their “arguments” – exposing the evaluator to their influence and efforts at manipulation of the evaluator’s opinion. This is a deeply concerning assessment process because of its vulnerability to the unconscious biases of the evaluator (called counter-transference in clinical psychology).
Counter-transference (unconscious bias) from the psychologist ALWAYS exists, in all cases, in all contents. The introduction of the psychologists own unconscious biases are identified as “schemas” in professional psychology. Personal biases in the assessment of information is always present, and is entirely unconscious to the person. This is a fact of psychology, and of all assessment processes.
In the forensic psychology process, the custody evaluator acts as the “judge” regarding the relative arguments offered by each parent, and they custody evaluator makes a determination of fact – typically whether a poorly defined construct called “parental alienation” is present and to what degree – and decides on the remedy based in the child’s custody visitation schedule with each parent.
Note: There is no pathology known as “parental alienation” in clinical psychology. That is a new form of pathology that is entirely the construction of forensic psychology. It does not exist. In clinical psychology, defined knowledge exists, and the identification of pathology (called diagnosis) is based solely on the established constructs and principles of professional psychology (attachment; family systems therapy; personality disorder pathology; complex trauma).
The focus on the treatment of family pathology, on the other hand, will move this into clinical psychology and a clinical psychology assessment of pathology.
Which legal argument and remedy package to present to the court is a decision for parents and their attorneys.
The Challenge of the Forensic Psychology Argument
The focus of the forensic psychology argument for the targeted parent is to prove a pathology (“parental alienation”) to a judge in order to obtain the remedy, typically a reversal of custody from the supposedly “favored” parent to the currently rejected targeted parent.
That is the burden, proving the family pathology of “parental alienation” to a judge at trial. The sole means to prove “parental alienation” to a judge at trial is through a forensic psychology child custody evaluation. A child custody evaluation costs between $20,000 to $40,000 and takes between six- to nine-months to complete.
There is no other option from the forensic psychology legal argument package. No second opinion is available because of the expense ($20,000 to $40,000) and length of time required (six to nine-months) for a child custody evaluation.
This approach is hardly ever successful for the targeted parent. This approach typically takes years of litigation and potentially hundreds of thousands of dollars in legal costs, with substantial damage to both the parent-child relationship and the family’s financial foundations during and throughout the years of litigation required by the forensic psychology approach.
Successful resolution of the family conflict is exceedingly rare using the forensic psychology legal argument package, because it’s not a treatment focused approach. Treatment is clinical psychology, and a clinical psychology assessment of pathology has not been conducted.
The forensic psychology approach typically only achieves success in the most severe cases of “parental alienation” in which the pathology of parental influence on the child is clearly evident, and then only after years of conflict and litigation have already robbed the child of a normal-range and healthy parent-child relationship with a loving and beloved parent (their mom or their dad; the targeted parent), and the loss of a normal-range childhood of healthy emotional and psychological development (bonded in loving relationships with both parents).
The forensic psychology approach offers no solution, it is destructive of families and children’s healthy emotional and psychological development, and this approach needs to change – because it offers no solution. It is not treatment focused. Treatment of child and family pathology is the domain of clinical psychology.
Clinical Psychology Argument
Clinical psychologists create change. We create change in individuals (individual therapy) and we create change in families (family therapy). Clinical child and family psychologists solve complex family conflict. That’s what we do. We solve complex family conflict. It’s called family systems therapy. Solving complex attachment-related family pathology surrounding divorce requires a solution from clinical psychology.
Clinical psychology can absolutely – 100% – solve this family pathology (cross- generational coalition; emotional cutoff; narcissistic-borderline parent (“splitting”); multigenerational transmission of complex trauma).
generational coalition; emotional cutoff; narcissistic-borderline parent (“splitting”); multigenerational transmission of complex trauma).
The solution requires the application of professional knowledge from four domains of professional psychology: the attachment system, family systems therapy, personality disorder pathology, and complex trauma. So it is not easy to solve. But it is entirely solvable with the application of the established knowledge of professional psychology.
Attachment – family systems therapy – personality disorder pathology – complex trauma. Established knowledge in professional psychology. Bowlby – Minuchin – Beck – van der Kolk.
I have posted a Curriculum Knowledge Checklist to my website that identifies the books from professional psychology that contain the professional knowledge needed to solve complex family conflict surrounding divorce.
It is a complex and difficult pathology. But it is both understandable and solvable.
Court Involvement
Solving this pathology will require a cooperative relationship between clinical psychology and the Court. The narcissistic-borderline parent will lead this family conflict into the court system by manipulatively creating and then exploiting the child’s refusal to comply with court orders for custody and visitation. Once the child begins refusing visitation contact with the targeted parent (with the tacit support of the allied narcissistic-borderline parent), the targeted-rejected parent must then return to court seeking enforcement of the existing court orders for custody and visitation.
That’s how the pathology of one spouse-and-parent (the allied parent who forms a cross-generational coalition with the child) drives the post-divorce family into the family court system. The family pathology will enter the legal system because the targeted parent needs to seek enforcement of the existing court orders for custody and visitation as a consequence of the child’s (manipulated and psychologically coerced) refusal to cooperate with the court orders for custody and visitation.
Since the issue is superficially the enforcement of orders for child custody and visitation, the issue will present to the court as one of “child custody” – but it’s not about custody and visitation. Court orders already exist. It’s about parental pathology in the family creating attachment-related pathology in the child in order to exploit the child’s symptoms to manipulate the court’s orders for custody and visitation (using the pathology – the rejection of a parent – created in the child).
This is a family pathology issue. That’s the domain of clinical psychology.
Victimized Child – Influenced Child
Upon entry into the legal system, the narcissistic-borderline parent will present the “victimized child” argument to the court; that the child is supposedly being “victimized” by the allegedly “abusive” parenting of the targeted parent, and the remedy sought by the allied narcissistic-borderline personality parent will be to severely limit the other parent’s time with the child ostensibly to limit the child’s contact with the supposedly “abusive parent.”
The targeted parent, on the other hand, will present the court with the “influenced child” argument surrounding the child’s refusal of contact, and the targeted parent will seek the remedy of limiting and restricting the the child’s time with the allied and “favored” in order to resolve the “influenced child” refusal of the court-ordered custody and visitation.
The judge will need to resolve between these two argument packages; “victimized child” offered by the allied and supposedly “protective” parent, and the “influenced child” argument offered by the targeted and rejected parent. Once the judicial decision is made regarding the arguments, an appropriate remedy will then need to decided upon by the Court.
Adjusting the Argument Package
The clinical psychology argument package adjusts both the focus (treatment of family pathology rather than child custody schedules) the the framing for how the “influenced child” argument is presented to the court.
The clinical psychology argument will NOT use the construct of “parental alienation” – and indeed, the use of the construct of “parental alienation” would be considered beneath professional standards of practice in clinical psychology. In clinical psychology, if a psychologist wants to apply a “new form of pathology” (such as “parental alienation”) to the interpretation of symptoms, this is done only AFTER having applied the standard and established knowledge of professional psychology; the attachment system literature, constructs from family systems therapy, personality disorder pathology, complex trauma, and the DSM diagnostic system. After.
The clinical psychology argument does NOT use the construct of “parental alienation” (because this construct is non-supported in the scientific literature of professional psychology), and is instead based entirely and solely on the solidly established constructs and principles of professional psychology (the attachment system, family systems therapy, personality disorders, complex trauma) – (Bowlby, Minuchin, Beck, van der Kolk, Millon, Kernberg, Perry, Haley, Bowen, Madanes, Linehan, Ainsworth…) – the standard and established knowledge of professional psychology applied to the symptom features of the pathology.
Up until now, the only option available to targeted parents and the court for obtaining input from professional psychology surrounding complex family conflict has been through forensic psychology and a child custody evaluation regarding the structure of the child custody schedule – and NOT the resolution of the family pathology issue.
The legal argument presented to the court is changing – from a forensic psychology package to a clinical psychology legal argument package. Parents and their attorneys are now beginning to ask for a clinical psychology assessment of family pathology; the pathology that is creating the complex family conflict that has entered the legal system.
The narcissistic-borderline parent has forced the targeted parent to return to court to seek enforcement of the existing child custody orders because the child has become severely symptomatic and non-cooperative with the established custody visitation schedule. This is the manipulative set-up by the narcissistic-borderline spouse-and-parent to make this about custody and visitation, driving the conflict into a forensic psychology approach focused on child custody (possession of the child) rather than a clinical psychology approach of diagnosis and treatment of pathology.
That is changing. An alternative legal argument package is available from clinical psychology for a treatment-focused assessment of the family. The referral question for the clinical psychology assessment is:
Referral Question: Which parent is the source of pathogenic parenting creating the child’s attachment-related pathology, and what are the treatment implications?
This clinical psychology referral question can be answered by a limited-scope clinical psychology assessment, typically requiring about six sessions and costing approximately $2,500 to complete. It is structured around two symptom documentation instruments, the Diagnostic Checklist for Pathogenic Parenting and the Parenting Practices Rating Scale.
The relatively low cost (~ $2,500) and short time frame (six to eight weeks) for the clinical psychology assessment allows for a second opinion assessment if desired, and the use of structured symptom documentation instruments (the Diagnostic Checklist and Parenting Practices Scale) allows for easy and clear comparison of findings from a first and second opinion report from clinical psychology.
The targeted parent is still offering the “influenced child” argument to the court, but is changing how that argument is structured and presented for the court’s consideration. Instead of using the incredibly weak construct of “parental alienation” that will drive the assessment into forensic psychology, the clinical psychology argument is solidly grounded in the established knowledge of professional psychology: the attachment system, complex trauma, and family systems therapy.
Of note is that the clinical psychology argument package to the court will not be using the personality disorder information sets from professional psychology in the argument presented to the court. The personality pathology information from professional psychology will emerge over time within the broader background understanding within the legal and mental health systems form gradually increasing familiarity with the pathology.
From the perspective of a clinical psychology family therapy solution, we do not want to emphasize the other parent’s pathology. There are other ways. Identifying pathology is important, because diagnosis guides treatment – but diagnosis is only important because it guides treatment. We do not want our focus to be on diagnosis, but on treatment. We want to pivot as quickly as we can away from identifying pathology (the diagnosis) and over to treatment.
The clinical psychology approach is solution focused; not problem driven. How do we fix things, how do we restore healthy parent-child bonds of affection, how do we restore the child’s normal-range and healthy childhood development? Solution focused.
What’s the pathology? A cross-generational coalition and emotional cutoff (attachment pathology). Minuchin’s diagram provides strong support for this argument. It displays exactly the pathology of concern.
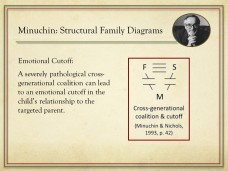
The Family Pathology: The child’s “triangulation” into the spousal conflict through the formation of a “cross-generational coalition” with the allied parent against the targeted parent, resulting in an “emotional cutoff” of the child’s relationship to the targeted parent (Minuchin; Haley; Bowen; Madanes; family systems therapy).
This type of family pathology is caused by “multigenerational trauma” (Bowen), also referred to as the trans-generational transmission of trauma in the attachment and complex trauma literature (Bowlby; van der Kolk).
The clinical psychology argument package presented to the court is that significant family pathology is resulting in the obstruction of court orders for custody and visitation. The remedy sought by the targeted parent is a treatment focused, trauma-informed, clinical psychology assessment of the family pathology.
That’s quite the mouthful for the assessment description.
Treatment Focused: The “treatment focused” indicator shifts the focus of the assessment off of the false child custody issue over to identifying a treatment oriented solution for the complex family conflict (through a written treatment plan for the resolution of child and family pathology; identified by the assessment).
Trauma Informed: The indicator of “trauma-informed” ensures that proper information sets from professional psychology are applied by the assessment.
Clinical Psychology: The clinical psychology orientation is to move the family conflict out of forensic psychology that offers no solution and over to the clinical psychology for the identification (diagnosis) and treatment of the (“high-conflict”) pathology in the family.
The initial remedy sought is:
Initial Remedy: A treatment-focused, trauma-informed, clinical psychology assessment of complex family conflict surrounding divorce.
The clinical psychology referral question is:
Referral Question: Which parent is the source of pathogenic parenting creating the child’s attachment-related pathology, and what are the treatment implications?
The focus is NOT child custody (which parent should “possess” the child following the divorce), it’s treatment. How do we restore normal-range and healthy child development? The targeted parent is making a treatment-focused argument to the court; that the custody violations to the court orders are a symptom of family pathology, and the targeted parent is seeking a clinical psychology assessment of the family pathology (along with the enforcement of existing court orders for custody and visitation) as the remedy.
This clinical psychology argument package effectively nullifies the “victimized child” argument offered by the narcissistic-borderline parent, since the treatment-focused, trauma-informed, clinical psychology assessment addresses the arguments from each parent and provides remedy for both.
If the child is indeed being “victimized” by the “abusive” parent (thereby justifying the child’s reluctance to be with the rejected parent) as is alleged by the allied parent and child, then a trauma-informed, treatment focused assessment from clinical psychology is just the assessment to identify this child “abuse” and “victimization” of the child by the targeted parent.
The narcissistic-borderline parent is using (exploiting) the child’s induced pathology (the child’s rejection of a mother or father) to make the issue about child custody (“possession” of the child following divorce; who’s the “better parent” that “deserves” possession of the child).
The targeted parent is using the child’s pathology created by the other parent to make the issue about the diagnosis and treatment of pathology. Since both agree on the existence of pathology, just not its causal source, a clinical psychology assessment and diagnosis, with treatment implications, is entirely warranted as the initial remedy for both arguments. Let’s find out what’s causing the child’s attachment-related pathology following the divorce – that’s a clinical psychology issue – identifying pathology is called diagnosis.
A clinical psychology argument package will extract targeted parents from the court system and return the assessment, diagnosis, and treatment of complex family conflict to clinical psychology, and it will prevent families with newly emerging divorce-related conflict from entering years of litigation in the family courts surrounding child custody, by making identification of the pathology in the family the first order from the court. Identify (diagnose) what is causing the child’s attachment-related pathology surrounding the divorce.
Initial Orders Sought for Remedy
Custody and visitation are not the focal point, they are symptom features of the complex family conflict. We need a treatment focused assessment from clinical psychology to determine what is going on, what the source for the complex family conflict is – using the standard and established knowledge of professional psychology (a trauma-informed assessment of complex family conflict).
A secondary remedy sought by the targeted parent is the enforcement of existing court orders for custody and visitation (and possibly sanctions on the allied parent for their responsibility in creating the breaches to the court orders).
In response to the clinical psychology argument package from the targeted parent, that carries a secondary remedy of enforcement and possible sanctions surrounding existing court orders for custody and visitation, the judge may decide to wait until the results of the clinical psychology assessment of family pathology before making a ruling on the custody orders from the court, and the judge will likely rule in favor of the targeted parent’s request for a “trauma informed, treatment focused, clinical psychology assessment of the complex family conflict.”
Second Opinion
The other party will likely argue against this clinical psychology assessment. The rebuttal to this argument that can be offered by the attorney for the targeted parent is “second opinion”; that the opposing party is free to obtain a second opinion, a second trauma-informed clinical psychology assessment of the complex family conflict.
If someone is concerned about a diagnosis in clinical psychology, get a second opinion. That’s how it’s done in clinical psychology (and health care generally). Get a second opinion if you’re concerned about the accuracy of diagnosis.
Child Protection Issue
That is the framing for the clinical psychology legal argument package.
The “custody” symptom (the child refusing court orders for custody and visitation) is a symptom of the family pathology. This is not a child custody issue, this is a child pathology issue. Is the targeted parent an “abusive” parent creating the child’s rejection, or is it the allied parent who is creating the child’s pathology through pathogenic parenting of psychological control and manipulation?
The referral question for the (“trauma-informed”) clinical psychology assessment is:
Referral Question: Which parent is the source of pathogenic parenting creating the child’s attachment-related pathology, and what are the treatment implications?
If the pathogenic parenting of the allied parent is creating significant developmental pathology in the child (attachment system suppression; diagnostic indicator 1), personality disorder pathology in the child (narcissistic personality traits; diagnostic indicator 2), and delusional-psychiatric pathology (encapsulated persecutory delusion; diagnostic indicator 3), the DSM-5 diagnosis is V995.51 Child Psychological Abuse, Confirmed, and the considerations shift to child protection.
In all cases of child abuse, physical child abuse, sexual child abuse, and psychological child abuse, the professional standard of practice and duty to protect requires the child’s protective separation from the abusive parent. The child’s healthy development is then recovered and restored, and once stabilized, contact with the formerly abusive parent is reestablished with sufficient safeguards to ensure that the child abuse does not resume once contact is restored.
This is true for physical child abuse, this is true for sexual child abuse, this is true for psychological child abuse.
That’s the shift that is occurring. The legal argument package being presented to the court, both in it’s foundations (Bowlby, Minuchin, Beck) and in the remedy sought (a clinical psychology assessment; psychological child abuse diagnosis; protective separation period and treatment recovery) is shifting to a clinical psychology legal argument package of solution
The world is changing. An attachment-based and trauma-informed model of complex family conflict surrounding divorce represents the return of clinical psychology to court-involved practice.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857